Whatcom County Heroin Dependant Population Needs Assessment
HISTORY OF THE NEED
Heroin is the fastest acting opiate drug, according to the National Institute on Drug Abuse (2005). The drug is synthesized form of morphine, which is from the poppy plant. Heroin can be sold on the street in black or white forms (NIDA, 2005). Other substances are added into often add into street heroin. The user is often unaware of the strength of the dose. Heroin is most often injected or smoked.
Heroin addiction is not a new phenomenon—individuals have become dependent on heroin since it came on the market. The drug company Bayer began to sell heroin over the counter medicine in 1895 (Askwith, 1998). Heroin was marketed as a safe, non-addictive alternative for morphine in cough medicine. The Bayer Company accidentally developed a faster acting form of morphine (Askwith, 1998). The first heroin epidemic began in the turn of the century among housewives and children (“Hooked: Opium, Morphine and Heroin”). The Harrison Narcotics Tax Act of 1914 limited heroin use to prescription usage. Congress later banned all use of heroin in 1924 (“Hooked: Opium, Morphine and Heroin”).
DESCRIPTION OF HEROIN ADDICTION
The illegalization of heroin has not decreased access of heroin in the black market. The 2008 National Survey on Drug Use and Health conducted by the US Department of Health and Human Services research found
3.8 million Americans aged 12 or older reported trying heroin at least once during there
lifetimes, representing 1.5% of the population aged 12 or older. Approximately 453,000
(0.2%) reported past year heroin use and 213,000 (0.1%) reported past month heroin use.
How many individuals in Whatcom County currently use and abuse heroin? The specific number may be difficult to pinpoint. Not all individuals who use heroin may be connected to community resources. The National Survey on Drug Abuse suggests that 0.1% of the American population has used heroin in the last month. Out of Whatcom County population of 201,140 (US Census Bureau, 2010), an appropriate 20,114 Whatcom County residents have used heroin in the last. Personal interviews with professionals in the field reflect an increase trend in heroin usage.
Opiate addiction hurts our community. The damage of the drug can be seen in crime, high healthcare costs, homelessness, childhood abuse and neglect, domestic violence, overdose deaths and the spread of preventable diseases. Individuals who use inject heroin are at risk for contracting hepatitis C and HIV (NIDA, 2005). Between seventy to eighty percent of new hepatitis C infections are IV drug users, (NIDA, 2005).
Substance abuse has a high economic cost. The 2008 Whatcom County Comprehensive Behavioral Health Plan states
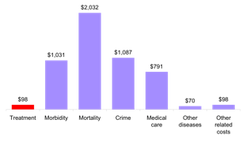
The costs of substance abuse are substantial: mortality, crime, and morbidity-related costs represented the largest economic costs of substance abuse in 2005. The estimated cost per death measured in terms of lost income was $630,000. Medical care costs ($791 million) – including hospital, outpatient medical care, prescription drugs, nursing homes, and other professional costs – were almost four times what they were in 1996 ($211 million).
The Comprehensive Behavioral Health Plan published a graph to show the general economic costs of drug and alcohol abuse in Washington State in 2005. The numbers are in the billions. It is interesting to compare the costs of addiction treatment to morbidity, crime and mortality costs. Substance abuse treatment cost much less money in Washington than the costs of other factors.
Heroin is cheap and easily acquirable in Bellingham, Washington. Dennis Whelan, manager at Whatcom County Social Detox (personal communication, April 5, 2011) reports “one gram of heroin, the amount that most people can prevent withdrawal is about thirty dollars.” Compared to the street cost of OxyContin, which costs eighty dollars per pill and most people use, several pills to get high a day, according to Dennis Whelan. “A few years ago heroin addicts were only a quarter of the detox client population; now they make more than one half” (D. Whelan, personal communication, April 5, 2011). Additional study needs to be done to understand the growth of heroin usuage.
What is the face of heroin users in Whatcom County? Current data and interviews of individuals in the field show that the face of a heroin addict residing in Whatcom County is likely a young person. Many addicts may enter the helping system through the police, jails/prison, Department of Social and Health Services, Emergency Room, and Detox centers prior to entering treatment. Wendy Jones, the Whatcom County Chief of Corrections reported to the Western Front News Paper (2010)
Heroin is the fastest acting opiate drug, according to the National Institute on Drug Abuse (2005). The drug is synthesized form of morphine, which is from the poppy plant. Heroin can be sold on the street in black or white forms (NIDA, 2005). Other substances are added into often add into street heroin. The user is often unaware of the strength of the dose. Heroin is most often injected or smoked.
Heroin addiction is not a new phenomenon—individuals have become dependent on heroin since it came on the market. The drug company Bayer began to sell heroin over the counter medicine in 1895 (Askwith, 1998). Heroin was marketed as a safe, non-addictive alternative for morphine in cough medicine. The Bayer Company accidentally developed a faster acting form of morphine (Askwith, 1998). The first heroin epidemic began in the turn of the century among housewives and children (“Hooked: Opium, Morphine and Heroin”). The Harrison Narcotics Tax Act of 1914 limited heroin use to prescription usage. Congress later banned all use of heroin in 1924 (“Hooked: Opium, Morphine and Heroin”).
DESCRIPTION OF HEROIN ADDICTION
The illegalization of heroin has not decreased access of heroin in the black market. The 2008 National Survey on Drug Use and Health conducted by the US Department of Health and Human Services research found
3.8 million Americans aged 12 or older reported trying heroin at least once during there
lifetimes, representing 1.5% of the population aged 12 or older. Approximately 453,000
(0.2%) reported past year heroin use and 213,000 (0.1%) reported past month heroin use.
How many individuals in Whatcom County currently use and abuse heroin? The specific number may be difficult to pinpoint. Not all individuals who use heroin may be connected to community resources. The National Survey on Drug Abuse suggests that 0.1% of the American population has used heroin in the last month. Out of Whatcom County population of 201,140 (US Census Bureau, 2010), an appropriate 20,114 Whatcom County residents have used heroin in the last. Personal interviews with professionals in the field reflect an increase trend in heroin usage.
Opiate addiction hurts our community. The damage of the drug can be seen in crime, high healthcare costs, homelessness, childhood abuse and neglect, domestic violence, overdose deaths and the spread of preventable diseases. Individuals who use inject heroin are at risk for contracting hepatitis C and HIV (NIDA, 2005). Between seventy to eighty percent of new hepatitis C infections are IV drug users, (NIDA, 2005).
Substance abuse has a high economic cost. The 2008 Whatcom County Comprehensive Behavioral Health Plan states
The costs of substance abuse are substantial: mortality, crime, and morbidity-related costs represented the largest economic costs of substance abuse in 2005. The estimated cost per death measured in terms of lost income was $630,000. Medical care costs ($791 million) – including hospital, outpatient medical care, prescription drugs, nursing homes, and other professional costs – were almost four times what they were in 1996 ($211 million).
The Comprehensive Behavioral Health Plan published a graph to show the general economic costs of drug and alcohol abuse in Washington State in 2005. The numbers are in the billions. It is interesting to compare the costs of addiction treatment to morbidity, crime and mortality costs. Substance abuse treatment cost much less money in Washington than the costs of other factors.
Heroin is cheap and easily acquirable in Bellingham, Washington. Dennis Whelan, manager at Whatcom County Social Detox (personal communication, April 5, 2011) reports “one gram of heroin, the amount that most people can prevent withdrawal is about thirty dollars.” Compared to the street cost of OxyContin, which costs eighty dollars per pill and most people use, several pills to get high a day, according to Dennis Whelan. “A few years ago heroin addicts were only a quarter of the detox client population; now they make more than one half” (D. Whelan, personal communication, April 5, 2011). Additional study needs to be done to understand the growth of heroin usuage.
What is the face of heroin users in Whatcom County? Current data and interviews of individuals in the field show that the face of a heroin addict residing in Whatcom County is likely a young person. Many addicts may enter the helping system through the police, jails/prison, Department of Social and Health Services, Emergency Room, and Detox centers prior to entering treatment. Wendy Jones, the Whatcom County Chief of Corrections reported to the Western Front News Paper (2010)
“Over the past three or four years, for the county jail, we are seeing a significant rise in
offenders under the influence of opiates, especially heroin,” said Wendy Jones, Whatcom
County Chief of Corrections. “They are people in their late teens to mid-20s, which is atypical
for [the county].”
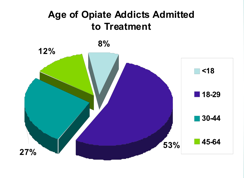
The graph on the right shows the age of Whatcom County Opiate Addicts entering treatment (Whatcom County Health Department), 2010. It should be noted that fifty-three percent of people admitted to treatment was under the age of twenty-nine. This data suggests the majority of heroin users are young adults. “Teenagers graduate from abusing prescription opiates like Percocet that they steel from their parents…their dependency develops and heroin is just a cheaper and faster high”, Jackie Mitchell explained in a phone interview (personal communication, April 10, 2011). Dennis Whelan believes that the quality, purity and accessibility of the drug are another reason for youth usage (personal communication, April 5, 2011).
UNMET NEED
Statistics on Whatcom County out-comes are not positive. Whatcom County ranks as the third Washington State County in need for more substance abuse services out of 39 counties (WCCBHP, 2008). The major stumbling block for individuals to stop active use of drugs is the ability to gain treatment access. The 2008 Whatcom County Comprehensive Behavioral Health Plan quotes several studies that show lower rates of access to treatment. 7,389 Whatcom residents needed treatment and only 1,360 accessed treatment services (DSHS, 2005).
Whatcom County’s ranked 32nd of 39 counties in the ability to provide treatment (WCCBHP, 2008). The uninsured population struggle to fund treatment. This population often relies on state healthcare coupon or applies for the Alcohol and Drug Abuse Treatment and Support Act. Jackie Mitchell, the Whatcom County Substance Abuse Programs Coordinator explains the need for Whatcom County low-income chemical dependant individuals (WCCBHP, 2008)
Only 24 of the 4,240 lower-income households that would benefit form community based
substance abuse are accessing it. Current policies force us to ration these service to the
indigent. There not enough funds to help provide these services to the indigent. There are
not enough funds help provide these services of the working poor and other poorly service
subgroups.
Those who do qualify for ADATSA program, 30% were never admitted to treatment at all (DSHS, 2007).
GAPS IN KNOWLEDGE
The opiate dependent population has unique needs compared dependant populations. Only 40% of opiate addicts completed their Social Detox stay compared to the 75% of alcohol and other drug addicts, according to 2009 Whatcom County Profile of Opiate Addiction. Opiate addicts left the program against medical double the amount of people abusing other chemicals (WCPOA, 2009). Evidence shows that detoxification stage of treatment is difficult for opiate addicts. If people leave against advice, rarely do they follow service recommendations.
A short survey study of Social Detox Center clients’ may bring further understanding of why opiate addicts are leave treatment early. Sample study questions should explore the reason why someone is leaving against medical advice. Do you plan on using? Would you be interested in gaining other possible treatment options? Are you aware of the steps that are needed to gain chemical dependency treatment? Have you bought suboxone on the street to stop withdrawal symptoms? Would you be interested in a suboxone program? Rate the likelihood of you following service providers’ recommendations. Another important aspect of a survey would explore individuals’ awareness of other countywide programs that serve intravenous drug users.
POTENTIAL SOLUTIONS
Dennis Whelan (personal communication, April 5, 2011) and Jackie Mitchell (personal communication, April 10, 2011) report that opiate addicts do not respond well to traditional treatment. Whatcom County is not doing well in providing appropriate interventions compared to other Washington State Counties. One barrier is limited amount of outpatient treatment options that serve low-income and uninsured individuals in Whatcom County. Distance is another barrier to treatment. Individuals who live in rural areas must commute to the Bellingham to receive services. The amount of Whatcom County does not have a local inpatient treatment program since Saint Joseph Hospital canceled its program a few years ago.
One potential solution is the development of a program that provides medical supervised maintenance. 2010 Whatcom County Needle Exchange Survey found that 95% of participants using heroin reported an interested in supervised withdrawal from opiates. The use of maintenance programs is not without its critics. Methadone and suboxone is currently the two types of medicine used for medical maintenance and withdrawal prevention (Wesson & Smith, 2010). Both substances work differently. Wesson and Smith (2010) report that Suboxone is better treatment option than methadone. Suboxone is less likely to cause overdose and abuse than methadone (Wesson & Smith, 2010). Jackie Mitchell reports that suboxone is more expensive than methadone (personal communication, April 10, 2011). Suboxone medicine is only a few years old.
Whatcom County does not have a Methadone program or suboxone program for low-income individuals. The Lummi Nation has a suboxone program only to tribal members (Dennis Whelan, personal interview, April 5, 2011). Currently suboxone is only available to high-income individuals or people who buy it off the black market (Jackie Mitchell, personal interview, April 10, 2011). Whatcom County currently does not have a physician willing to prescribe methadone. The closest methadone program is in Snohonomish County. Dennis Whelan reports that he knows of individuals who commute to Arlington, WA for daily methadone doses (personal communication, April 5, 2011). Heroin addicts may benefit from a low cost suboxone or methadone program—further research in best practices is needed.
References
Askwith, R. (1998, September 13). How aspirin turned hero. Sunday Time. Retrieved from
http://opioids.com/heroin/heroinhistory.html.
Department of Social and Health Services. (2007). Tobacco, alcohol, and other drug abuse
trends in Washington state.
Department of Social and Health Services Research and Data Analysis Division (2005). County
profile of substance use and need for treatment services: Whatcom county.
Sawyer, J. (2010, November 23). Heroin on the rise among Whatcom youth, police say. Western
Front. Retrieved from
http://westernfrontonline.net/news/12861-heroin-on-the-rise-among-whatcom-youth-police-say
National Institute on Drug Abuse (2005). Research Report Series - Heroin Abuse and Addiction
http://www.nida.nih.gov/ResearchReports/Heroin/heroin2.html#what
Substance Abuse and Mental Health Services Administration. (2009). Results from the 2008
National Survey on Drug Use and Health: National Findings (Office of Applied Studies,
NSDUH Series H-36, HHS Publication No. SMA 09-4434). Rockville, MD.
United States Census Bureau. (2010). Whatcom County Quick facts. Retrieved from
http://quickfacts.census.gov/qfd/states/53/53073.html
Wesson, D. R., & Smith, D. E. (2010). Buprenorphine in the Treatment of Opiate Dependence.
Journal of Psychoactive Drugs, 42(2), 161-175.
Whatcom County Health Department. (2010). Whatcom County Needle Exchange Survey.
Bellingham, WA. Retrieved from personal e-mail with Jackie Mitchell.
Whatcom County Health Department. (2010). Whatcom County Profile of Opiate Addiction.
Bellingham, WA. Retrieved from personal e-mail with Jackie Mitchell.
Whatcom County Health Department. (2008). Whatcom County Comprehensive Behavioral
Health Plan. Retrieved from
http://www.co.whatcom.wa.us/health/pdf/comp_health_plan.pdf
(2005). Hooked: opium, morphine and heroin [in television episode]. In Hooked: illegal drugs
and how they got that way. Los Angeles: History Channel.
offenders under the influence of opiates, especially heroin,” said Wendy Jones, Whatcom
County Chief of Corrections. “They are people in their late teens to mid-20s, which is atypical
for [the county].”
The graph on the right shows the age of Whatcom County Opiate Addicts entering treatment (Whatcom County Health Department), 2010. It should be noted that fifty-three percent of people admitted to treatment was under the age of twenty-nine. This data suggests the majority of heroin users are young adults. “Teenagers graduate from abusing prescription opiates like Percocet that they steel from their parents…their dependency develops and heroin is just a cheaper and faster high”, Jackie Mitchell explained in a phone interview (personal communication, April 10, 2011). Dennis Whelan believes that the quality, purity and accessibility of the drug are another reason for youth usage (personal communication, April 5, 2011).
UNMET NEED
Statistics on Whatcom County out-comes are not positive. Whatcom County ranks as the third Washington State County in need for more substance abuse services out of 39 counties (WCCBHP, 2008). The major stumbling block for individuals to stop active use of drugs is the ability to gain treatment access. The 2008 Whatcom County Comprehensive Behavioral Health Plan quotes several studies that show lower rates of access to treatment. 7,389 Whatcom residents needed treatment and only 1,360 accessed treatment services (DSHS, 2005).
Whatcom County’s ranked 32nd of 39 counties in the ability to provide treatment (WCCBHP, 2008). The uninsured population struggle to fund treatment. This population often relies on state healthcare coupon or applies for the Alcohol and Drug Abuse Treatment and Support Act. Jackie Mitchell, the Whatcom County Substance Abuse Programs Coordinator explains the need for Whatcom County low-income chemical dependant individuals (WCCBHP, 2008)
Only 24 of the 4,240 lower-income households that would benefit form community based
substance abuse are accessing it. Current policies force us to ration these service to the
indigent. There not enough funds to help provide these services to the indigent. There are
not enough funds help provide these services of the working poor and other poorly service
subgroups.
Those who do qualify for ADATSA program, 30% were never admitted to treatment at all (DSHS, 2007).
GAPS IN KNOWLEDGE
The opiate dependent population has unique needs compared dependant populations. Only 40% of opiate addicts completed their Social Detox stay compared to the 75% of alcohol and other drug addicts, according to 2009 Whatcom County Profile of Opiate Addiction. Opiate addicts left the program against medical double the amount of people abusing other chemicals (WCPOA, 2009). Evidence shows that detoxification stage of treatment is difficult for opiate addicts. If people leave against advice, rarely do they follow service recommendations.
A short survey study of Social Detox Center clients’ may bring further understanding of why opiate addicts are leave treatment early. Sample study questions should explore the reason why someone is leaving against medical advice. Do you plan on using? Would you be interested in gaining other possible treatment options? Are you aware of the steps that are needed to gain chemical dependency treatment? Have you bought suboxone on the street to stop withdrawal symptoms? Would you be interested in a suboxone program? Rate the likelihood of you following service providers’ recommendations. Another important aspect of a survey would explore individuals’ awareness of other countywide programs that serve intravenous drug users.
POTENTIAL SOLUTIONS
Dennis Whelan (personal communication, April 5, 2011) and Jackie Mitchell (personal communication, April 10, 2011) report that opiate addicts do not respond well to traditional treatment. Whatcom County is not doing well in providing appropriate interventions compared to other Washington State Counties. One barrier is limited amount of outpatient treatment options that serve low-income and uninsured individuals in Whatcom County. Distance is another barrier to treatment. Individuals who live in rural areas must commute to the Bellingham to receive services. The amount of Whatcom County does not have a local inpatient treatment program since Saint Joseph Hospital canceled its program a few years ago.
One potential solution is the development of a program that provides medical supervised maintenance. 2010 Whatcom County Needle Exchange Survey found that 95% of participants using heroin reported an interested in supervised withdrawal from opiates. The use of maintenance programs is not without its critics. Methadone and suboxone is currently the two types of medicine used for medical maintenance and withdrawal prevention (Wesson & Smith, 2010). Both substances work differently. Wesson and Smith (2010) report that Suboxone is better treatment option than methadone. Suboxone is less likely to cause overdose and abuse than methadone (Wesson & Smith, 2010). Jackie Mitchell reports that suboxone is more expensive than methadone (personal communication, April 10, 2011). Suboxone medicine is only a few years old.
Whatcom County does not have a Methadone program or suboxone program for low-income individuals. The Lummi Nation has a suboxone program only to tribal members (Dennis Whelan, personal interview, April 5, 2011). Currently suboxone is only available to high-income individuals or people who buy it off the black market (Jackie Mitchell, personal interview, April 10, 2011). Whatcom County currently does not have a physician willing to prescribe methadone. The closest methadone program is in Snohonomish County. Dennis Whelan reports that he knows of individuals who commute to Arlington, WA for daily methadone doses (personal communication, April 5, 2011). Heroin addicts may benefit from a low cost suboxone or methadone program—further research in best practices is needed.
References
Askwith, R. (1998, September 13). How aspirin turned hero. Sunday Time. Retrieved from
http://opioids.com/heroin/heroinhistory.html.
Department of Social and Health Services. (2007). Tobacco, alcohol, and other drug abuse
trends in Washington state.
Department of Social and Health Services Research and Data Analysis Division (2005). County
profile of substance use and need for treatment services: Whatcom county.
Sawyer, J. (2010, November 23). Heroin on the rise among Whatcom youth, police say. Western
Front. Retrieved from
http://westernfrontonline.net/news/12861-heroin-on-the-rise-among-whatcom-youth-police-say
National Institute on Drug Abuse (2005). Research Report Series - Heroin Abuse and Addiction
http://www.nida.nih.gov/ResearchReports/Heroin/heroin2.html#what
Substance Abuse and Mental Health Services Administration. (2009). Results from the 2008
National Survey on Drug Use and Health: National Findings (Office of Applied Studies,
NSDUH Series H-36, HHS Publication No. SMA 09-4434). Rockville, MD.
United States Census Bureau. (2010). Whatcom County Quick facts. Retrieved from
http://quickfacts.census.gov/qfd/states/53/53073.html
Wesson, D. R., & Smith, D. E. (2010). Buprenorphine in the Treatment of Opiate Dependence.
Journal of Psychoactive Drugs, 42(2), 161-175.
Whatcom County Health Department. (2010). Whatcom County Needle Exchange Survey.
Bellingham, WA. Retrieved from personal e-mail with Jackie Mitchell.
Whatcom County Health Department. (2010). Whatcom County Profile of Opiate Addiction.
Bellingham, WA. Retrieved from personal e-mail with Jackie Mitchell.
Whatcom County Health Department. (2008). Whatcom County Comprehensive Behavioral
Health Plan. Retrieved from
http://www.co.whatcom.wa.us/health/pdf/comp_health_plan.pdf
(2005). Hooked: opium, morphine and heroin [in television episode]. In Hooked: illegal drugs
and how they got that way. Los Angeles: History Channel.
